Journal club: Martin et al, 2020
Enabling the future of colonoscopy with intelligent and autonomous magnetic manipulation
James W. Martin, Bruno Scaglioni, Joseph C. Norton,Venkataraman Subramanian, Alberto Arezzo, Keith L. Obstein, Pietro Valdastri
Nature Machine Intelligence (Volume: 2, September 2020)
DOI: http://doi.org/10.1109/LRA.2018.2812907
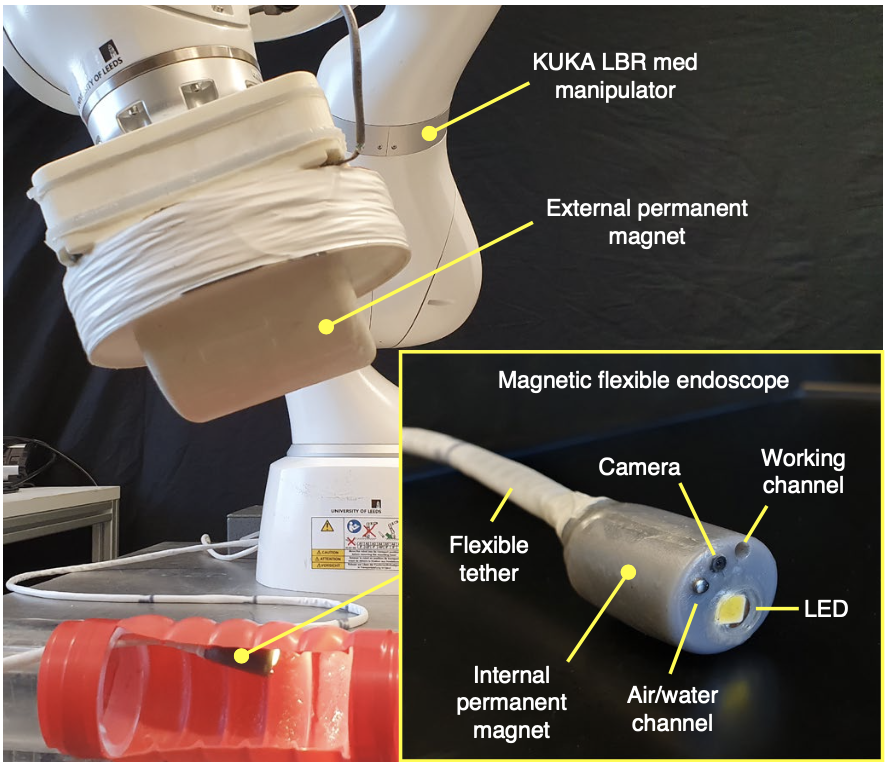
In this work, authors proposed a magnetic endoscope that can be controlled externally using a robotic arm such as the Kuka Robot that is equipped with a external permanent magnet. Refer to Fig. 1.
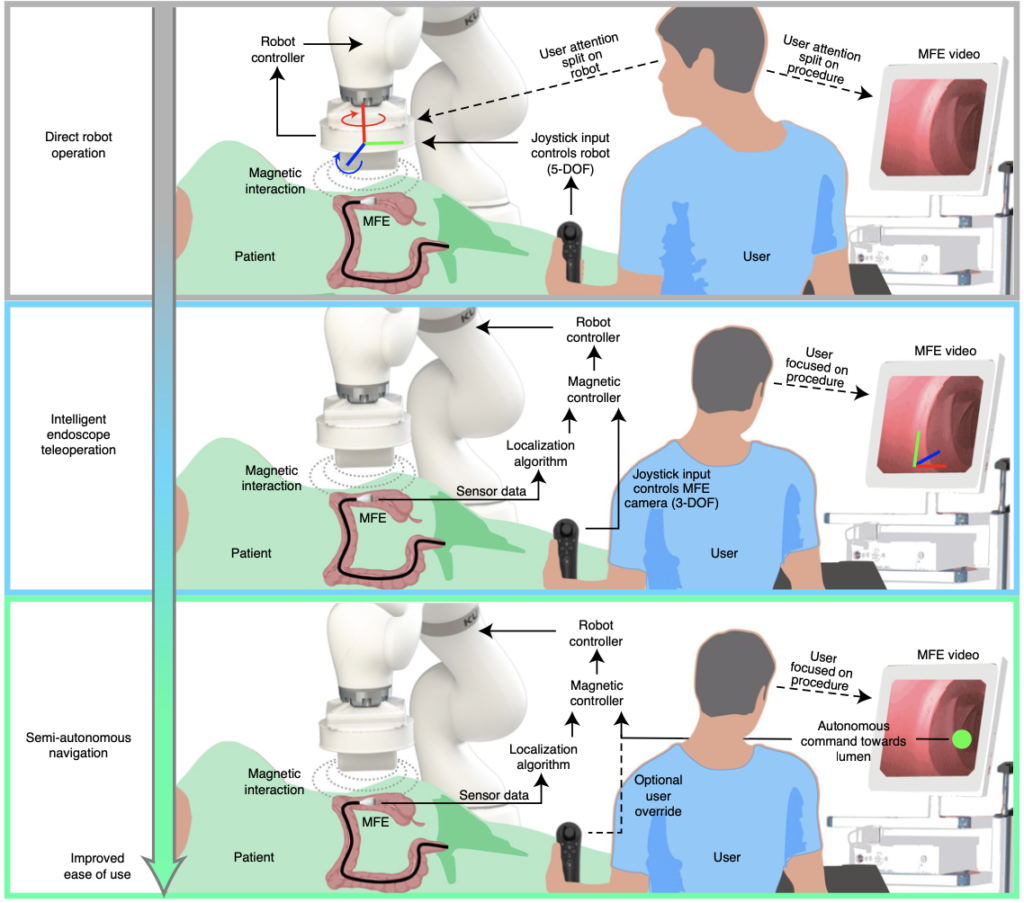
The hypothesis of this work is that controlling magnetically manipulated endoscopes by introducing superior levels of intelligence and autonomy could increase their navigational performance. Hence, the authors describe three levels of autonomy
- The first layer is called direct robot operation. Here, the user manually controls the robot end effector through a 5 DoF joystick to manipulate the magnetic endoscope, no autonomy. This represents an elementary level of manual control whereby the user must themselves control variations in the interacting magnetic fields. So, he/she has to split their attention between the robot control and the video feed from the endoscope.
- In the second layer, the user inputs are directly focused on navigating the endoscope through the colon, while the system carries the burden of generating a suitable magnetic control action to accomplish the desired endoscope motion. Here, the user has to stay focused on the screen, and system carries out the required motion for the robot. This layer is called intelligent endoscope teleoperation.
- In the third layer, the system detects the lumen and carries out the required motion. This layer is called semi-autonomous navigation and it puts the user in a discrete control of the endoscope, and the user can override if desired.
The authors validate their approach through benchtop and in-vivo experiments respectively. The work provides a demonstration of intelligent and autonomous control enabling non-expert users to successfully perform magnetic colonoscopy and with a duration comparable to standard FE. The study defines a framework to define the increasing levels of autonomy applied to robotic flexible endoscopy that have reduced the exertion of the user.
Discussion:
Following the presentation, ESRs discussed the results regarding the following points:
- Autonomous Navigation: ESRs working on path-planning approaches for the control of intraluminal procedures discussed of a common index/metrics used to determine the precision of the trajectories. In most cases, the trajectory taken by surgeon varies from surgeon to surgeon, however until the trajectory does not lead to complications such as perforation or bleeding, and roughly takes the average time, it is considered safe. Further discussion was carried out on pros and cons of planning methods such as Centerline method, Reinforcement learning
- Image processing algorithm: One of the main points remarked was that the experiments conducted in this paper used controlled environment such as synthetic phantoms, cleaned pig bowels. This reduces the noise that is usually found in colonoscopy scenarios. This point needs to be addressed with more realistic images.
- Actuation methods for magnetic endoscopy: One of important point commented were whether magnetic actuation could work in real clinical scenarios as magnetic endoscope requires high bending forces.
- There were questions raised in regard to the ethical aspects of the adoption of the superior levels of autonomous system.